



Exercise Addiction: Understanding How & Why It Happens
Exercise is often referred to as the ultimate drug, and unfortunately, it can also have drug like qualities as exercise addiction is very real. Given that physical exercise can increase strength, improve body composition and reduce the risk of metabolic diseases- it is often thought that there is no such thing as too much exercise. With the growing number of men and women across the globe who are over their ideal body weight and the increased inactivity that modern life imposes upon us, the call to exercise more is one that every major health and fitness related authority recommends. In a way, exercise is the drug that every doctor is keen to prescribe. A drug that comes seemingly without any adverse side effects, but the reality is that exercise, like everything else in life done to excess, does have a negative side, and that dark is the possibility of exercise addiction. In my practice as a personal trainer in New York City over the past 27 years, I have seen exercise addiction first hand among hundreds of athletes, gym goers and bodybuilders. Being aware that exercise addiction was a very real possibility for me as well was a factor in the creation of my own philosophy of implementing high intensity training only three times a week for no more than 10-20 minutes per workout session. The relative infrequency of the workouts has helped me and many of my clients not fall into the open trap of exercise addiction and has helped several athletes who one could easily identify as being exercise addicted find a balance in making training a healthy and non destructive part of their lives. In this article we explore not only what exercise addiction is, but how to tell if you are an exercise addict. As with any addiction, self identification is extremely difficult, much less pursuing treatments and behavioral changes on your own, but it is my hope that this article at least helps shed some light on the fact that exercise addiction is not only real, but pervasive in Western societies. Do be sure to share this article with anyone who you think might benefit from reading it!
Exercise, for most is a pleasurable activity and can the quest for that pleasure can be pursued without any consideration for the negative consequences it can inflict when done in excess. While one might be tempted to assume that any devoted or accomplished athlete must suffer from some form of exercise addiction, a comprehensive overview of what addiction is and how it relates to physical activity shows that this isn’t always the case. Some athletes and enthusiasts who regularly engage in intense physical exercise of any kind- be it weight training, yoga, bodybuilding, running, aerobics, athletics or martial arts training, may suffer from exercise addiction. However everyone who trains at an advanced level is not an exercise addict, as addiction has little to do with how much or how intensely you exercise.[1] In the following paragraphs we will take a look at the phases of exercise addiction and identify its occurrence while clearly distinguishing healthy exercise patterns from negative and addictive behaviors.
Exercise Addiction: Defining What Addiction Is And What It Isn’t

While the American Psychiatric Association’s Diagnostic & Statistical Manual of Mental Disorders (DSM-5) does not list exercise addiction as a separate disorder- it’s upcoming fifth edition does lay down criteria for what are known as behavioral addictions.[2] Exercise addition falls within the subset of behavioral additions and is quite distinct from healthy exercise habits. In order for a behavior to be classified as an addiction the following basic criteria must exist:
- Withdrawal Symptoms: When the activity is stopped the individual becomes anxious, irritable, restless and has difficulty sleeping. [6]
- Lack of Self Control: The individual has difficulty reducing the intensity or frequency of exercise or is unable to stop exercising for a certain period of time.
- Mood Modification: This refers to the subjective experiences that people report when exercising that can be seen as a coping strategy (i.e., they experience an arousing ‘‘buzz’’ or a ‘‘high’’, or paradoxically tranquilizing feel of ‘‘escape’’ or ‘‘numbing’’).[3]
- Increased Tolerance: The individual needs to keep increasing the volume, frequency or intensity of exercise in order to feel the desired effect- be it euphoria, a sense of accomplishment or increased self-esteem.
- Intention Effects: The individual is unable to stick to his or her intended routine and frequently trains longer than intended.
- Time: A significant amount of time is spent preparing for, recovering from or engaging in physical exercise.
- Continuance: Behavior where the individual continues to exercise in spite of the fact that he or she is aware that the activity is creating or exacerbating physical or interpersonal problems. For example- continuing to train in spite of serious injury, or breaking off relationships with loved ones in order to engage in the activity.
- Reduction In Other Activities: Behavior where social, occupational and or recreational activities are stopped as a direct result of physical exercise.[1]
- Relapse: In spite of significant time away from the addictive exercise activity, the tendency exists for the same patterns of addictive behavior to resurface. Even after years of abstinence and or control.
Exercise Addiction Is Not A Matter Of Intensity Or Frequency
Given the above criteria, what immediately stands out is that frequency and intensity are not qualifying features of exercise addiction. [4,5] An athlete preparing for a competition, for example, may devote a significant amount of time to the activity at hand while cutting back sharply on his or her non exercise or sport related activities. He or she may even experience some feelings of withdrawal at the end of the competitive cycle, when the frequency or intensity of training is reduced. However, even though several of the criteria for exercise addiction are met, this behavior does not necessarily constitute addiction, as there are other phases that must occur before a behavior can be categorized as addictive.
Exercise Addiction: The Steps Leading To Exercise Addiction
Originally thought to be an obsessive compulsive disorder (OCD), exercise addiction distinguishes itself from impulse control disorders in several important ways. With compulsive disorders the individual obsesses about performing ritualistic activity that revolves around unrealistic outcomes. Take the common OCD example of an individual who can’t stop washing their hands out of a need to remain germ free.[1] It’s not possible nor is it realistic to not have some germs on your hands, nor is it rational to spend significant amounts of time worrying about contracting disease from germs on your hands. In any case, the desired outcome of the obsessive behavior is unrealistic. Contrast this with the addict thinking about their next high and how they will feel as a result. In addiction, the individual ruminates about a very realistic, (although negative), outcome from his or her behavior, regardless of the consequences.[2] This, along with the development of tolerance, withdrawal symptoms and relapse readily separates exercise addiction from anxiety-related compulsive disorders. To determine behavior that can be classified as exercise addiction, it must conform with the following four phases of addiction.[3] Phases that are best illustrated by the following example:
Brianna found that she was putting on a few extra pounds and decides to join a gym with hopes of losing weight and getting in shape. Going to the gym every evening after work she discovers that she really enjoys how much her training program improves her strength and appearance and the way it makes her feel. The workouts help her forget the stress of her everyday life and provide a much needed break from some of her problems and worries. In time, a trainer at the gym suggests that she enters a bikini competition and so she increases her training to a routine of cardio and weight training twice a day for several months. After successfully competing and placing well in the show, she likes how she looks and feels and decides to continue training twice a day and she increases her time on the treadmill as it helps her keep her mind clear. Friends and family are concerned that she spends so much time in the gym and she is noticeably absent from important social gatherings if they occur during her scheduled gym times. Her knees and shins hurt but she ignores it thinking “no pain-no gain.”One day she feels a sharp pain in her ankle- she has suffered a severe sprain and her physician recommends that she stop training for a while. After the first day of not training she feels irritable and has a sense that something isn’t right. She misses training terribly and is becomes more and more depressed. Against medical advice, she returns to the gym to do some weight training, but several days later she decides to get back on the treadmill. She runs until her ankle gives out completely.
Exercise Addiction: Phase 1- Recreational Exercise

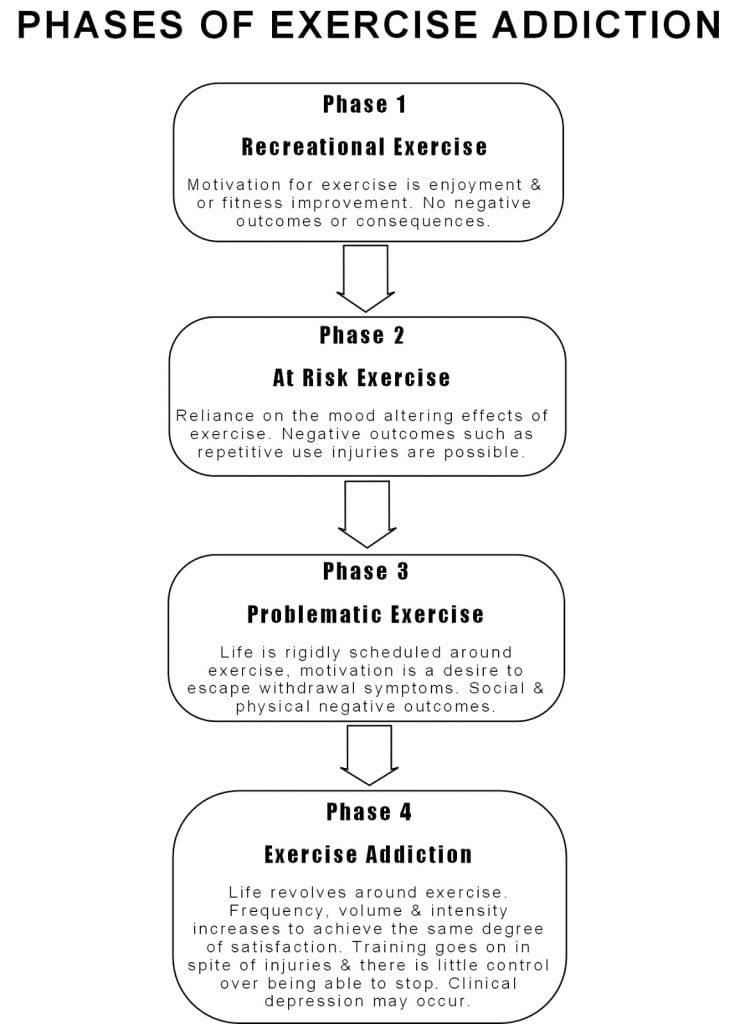
In the above example, Brianna goes through distinct phases on her way to developing behavior that can be defined as addictive. Phases that are key barometers of whether someone is engaged in healthy activity or negative addictive behavior. In the first phase there is Recreational Exercise, where Brianna’s primary motivation for training is an appreciation of the physical changes to her body and the pleasure that comes with physical activity. This behavior is under control with little or no risk of negative consequences, aside from manageable muscle soreness after the workout, and occurs within the parameters of the individual’s schedule. Such activity can be stopped at any time with little or no consequences. Unlike addictive behavior this phase of healthy recreational exercise enhances quality of life unlike exercise addiction which makes life unmanageable.[4]
Exercise Addiction: Phase 2 At Risk Exercise

In the second phase At Risk Exercise occurs. This happens when the individual discovers through recreational exercise that training can have a profound effect on his or her mood and self esteem. In the cited example, Brianna finds that she can temporarily escape the problems of her life while exercising and that she feels much better about herself as well. It is a well documented fact that exercise can increase self esteem and decrease the negative effects associated with depression and anxiety.[5] (See my article on Exercise & Depression). This mood altering effect occurs with both aerobic type activities such as running as well as anaerobic exercises such as weight training. ]6,7,8,9,10]
One commonly cited explanation is that during exercise our bodies release endorphins, which are naturally occurring opiates that create a feeling of euphoria and well being. ‘The runner’s high’ or the physical rush of feeling alive that is often described by those who push their bodies to the limit a regular basis. Unfortunately, with some individuals, over time the increased endorphin production from regular exercise results in a reduction (down-regulation) of the amount of endorphins produced while not exercising. Thus they feel compelled to exercise as a way of maintaining a natural balance in the brain. [4] Other proposed mechanisms explaining the connection between mood improvement and regular exercise are the thermogenic and catecholamine hypotheses. In the thermogenic hypothesis, the increase in body temperature is thought to be responsible for decreased anxiety.[11]) Whereas in the catecholamine hypothesis, catecholamines which are linked to changes in mood, alertness, movement, cardiovascular and hormonal responses, are thought to be the cause of elevated mood during physical activity. [12]
Regardless of the biology behind mood elevation, the problem lies in the individual’s primary motivation for exercising. With healthy physical activity, enjoyment of the activity and its benefits are the driving reasons to exercise. However with at risk exercise, motivation comes not from enjoyment of the activity but from the stress relief it creates, the improved self-esteem and relief from anger, depression and boredom.[4,13,14] Studies show that the likelihood of exercise addiction is far greater among those who exercise to escape negative feelings or change their appearance to improve self esteem as compared to those who train to improve fitness and performance.[4] The more physical activity becomes the sole means of relieving stress the more likely addiction is to occur.[35] The transition between at risk exercise is also marked by periods where negative physical consequences such as repetitive injuries become increasingly common. In the example given, Brianna’s ankle injury is a direct negative consequence of her extreme exercise routine.
Exercise Addiction Phase 3- Problematic Exercise

The third phase is known as Problematic Exercise and it occurs when the individual begins to rigidly schedule their daily lives around their exercise program. [32] In the example given, Brianna begins to miss more and more social events with friends and family, especially those that would interfere with her scheduled workouts. With problematic exercise the individual also tends to experience withdrawal symptoms, as evidenced by Brianna’s feelings of depression and irritability when she stops training temporarily due to injury. In this stage there is the beginning of a loss of control as the motivation to exercise becomes the desire to escape the withdrawal symptoms that come with stopping.
Exercise Addiction: Phase 4- Addiction

The fourth and final phase is Exercise Addiction. At this point life revolves around training and in spite of feeling the physical rush that comes with exercise, the individual continues to increase the volume, frequency or intensity of training- regardless of any negative outcomes. In the example, Brianna goes from someone who exercised to improve her life, to someone for whom exercise makes life almost unbearable as she feels compelled to train primarily to avoid dealing with the lows that come with withdrawal. So much so that it exacerbates the gravity of her ankle injury. At this stage there are almost always negative outcomes in the form of injuries and the inability to meet social obligations and role obligations. In many cases this behavior leads to clinical depression.[4]
Exercise Addiction Risk Factors: Why Do Some People Become Addicted?
Why some people succumb to exercise addiction while others do not is an important question to ask. Study reviews estimate that exercise addiction occurs in only 3% of the general population. [16] A figure that makes it relatively rare but its incidence has been found to be much higher among certain groups such as ultra-marathon runners and sports science students.[16,17,18] While there are no large scale studies conducted with this particular population, given the relationship between addictive behaviors and disorders among exercisers who have a high need for perfection and control over their bodies and lives,[4] I would assume the rate of exercise addition to be higher as well among competitive bodybuilders, fitness, figure and bikini competitors. A high incidence that my own personal experiences with individuals in the sport and among regular gym goers over the past two decades leads me to believe to be all too true. Rates of addiction have indeed found to be quite high among regular gym goers as one French study found 42% of the members of a club in Paris exhibiting signs of exercise addiction.[19] Research has shown that there are a number of risk factors that can predispose someone regularly involved in highly engaged levels of training to exercise addiction. Risk factors that hold true for any form of addiction such as genetic and neurological predispositions, negative peers, low self-esteem, juvenile delinquency, parental drug use and low levels of social conformity.[35]

Some research has shown that exercise addicted individuals also tend to have other addictive behaviors that co-occur with their exercise addiction. Buying addiction, work addiction and sex addiction has been identified as common among those addicted to exercise [19,20,21,22] and some estimate that 15-20% of exercise addicted individuals are addicted to nicotine, alcohol or illegal drugs.[23] Experts propose that addictions are seldom singular in nature and athletes suffering from exercise addiction are especially susceptible to developing or suffering from substance abuse related addictions using stimulants to improve performance and body composition such as amphetamines, ephedra, cocaine or caffeine. [24-25] The use of anabolic steroids has also been similarly linked to the use of cocaine and illicit substance abuse[26,27] and while there is little research available again my experience has been that some steroid users show very real signs of co-addictions and eating disorders.
Exercise Addiction & Eating Disorders
Eating disorders are the most common disorders that co-occur with exercise addiction with anywhere from 39-48% of people with eating disorders also suffering from exercise addiction.[28,29,36] For many the primary motivation for exercise is weight loss in the extreme- termed anoerxia athletica[37,31] and it is often paired with vomiting, use of laxatives and diet pills to avoid any potential weight gain from regular calorie consumption.[30]This is a very serious problem for many women, however it is becoming clear that men do suffer from eating disorders as well.[32] The problem is that while eating disorders are regularly diagnosed and treated, the co-occurring exercise addiction is often left unchecked. Repetitive injuries can often be a sign of exercise addiction, however they are usually not identified by clinicians as such due to the lack of material on hand regarding this form of addiction.
Treating Exercise Addiction
Treating exercise addiction is difficult and presents some very real practical challenges as unlike other addictions where abstinence is usually the ultimate goal, exercise is a positive activity and an important part of overall health. Thus in addition to several forms of cognitive therapy, the emphasis is on finding a balance and a return to moderate recreational exercise as opposed to stopping completely.[33] In some cases other forms of exercise may be suggested as well- for example a runner may be advised to take up swimming or a weight trainer advised to try hiking and other outdoor activities. Since exercise is often prescribed as a remedy for those suffering from depression, care must also be taken in ensuring that such at risk populations do not develop addictive behaviors by using exercise as their sole coping mechanism and by having physical activity dominate their lives. Essentially trading depression for a potentially harmful addiction. Nevertheless exercise remains a valuable tool in treating depression, but there is a need for more large scale studies documenting exercise addiction. It is hoped that this article will at the very least provide an overview of exercise addiction and help avid exercisers distinguish it from highly engaged forms of exercise. Like all addictions and disorders, if you do suspect that you have a problem, the earlier you get help the better the outcomes tend to be. It’s hard to look at a habit of regular exercise as a problem, but exercise can indeed sometimes be too much of a good thing.[34] Below is a standardized short form for basic evaluation of potential exercise addiction-
Click Here For A Basic Test For Exercise Addiction

{kind=link}
{kind=link}

High Intensity Bodyweight Training: Ballistic Pushups & Dips!
This was a tough one!
Starts out with ballistic push ups (like clap pushups but without the clap as my wrist is still not 100%) nonstop for 20 reps, then all out on dips for 10 reps.
To say it was painful would be an understatement, but you just have to push through and keep on going.
Still training, hope you are too and as always, Excelsior!!! #naturallyintense
#hometraining #homeworkout #homeworkout #highintensitytraining #naturalbodybuilder #naturalbodybuilding #fitover40 #naturalbodybuildingvideos #chestday #chesttraining #naturalbodybuildingtips #pushups #dips #bodyweighttraining #highintensitytrainingtips #drugfreebodybuilding #calesthenics
{kind=link}
Kevin's Unconventional Biceps Training- 3-6 Minutes a Week!
In this video I go over my biceps training using the Naturally Intense High Intensity Training protocols that helped me go from having arms measuring 11.5 to 12 inches to 18 inches drug free!
It's an unconventional approach for certain, but it's one that's helped my arms grow and the hundreds of men and women I have trained over the past 30 plus years.
Now, my success isn't due to being genetically gifted, as it took me the better part of 11 years to get my arms up to those measurements.
Which is significant as it works and been been proven time and time again to work for the average man or woman trying to grow their arms without drugs.
It's my hope that these high intensity training protocols can help you as much as they helped me!
Click on my bio link to see the full video on my YouTube channel and thanks as always for taking the time to look at my work!!! Excelsior!!! #naturallyintense
#highintensitytraining #naturalbodybuilder #naturalbodybuilding #fitover40 #naturalbodybuildingvideos #armworkout #bicepsworkout #naturalbodybuildingtips #biceps #armtraining #highintensitytrainingtips #drugfreebodybuilding #barbellcurls
{kind=link}
At the Lancaster Classic Day 2 Elimination Rounds Against European Champion, and World Record Holder Leo Pettersen @leo_barebow_archer
I don't talk much about it but I'm also a competitive barebow archer (surprise!) and last Saturday I had the honor of making it to Day 2 at the Lancaster Archery Classic in the Barebow Division, as I made the top 64 out of 267 competitors and had a chance to shoot with some of the greatest barebow shooters on the planet!
I didn't make it past Leo, but it was a real rush to be there and a huge thanks to my coach, Joe MyGlyn @prolinearchery for helping me get there.
Thanks as well to my good friend @sean_chan33 for all of his help from the very start, to my line buddy Aaron Shea for taking the shot and showing up to support!
My thanks as well to rob_kaufhold for putting on and promoting one of the best archery tournaments on earth!
Thanks also to to everyone who took the time to send a supporting word and I am looking forward to next year!!! #naturallyintense #barebow
#lancasterclassic #lancasterarcheryclassic2024 #lancasterarchery #archery #fitover40 #barebowrecurve #targetarchery
{kind=link}
Dumbo, Brooklyn circa 2004
This shot was taken as part of the promotion for my Naturally Intense DVD and was about a year after my last bodybuilding competition.
It was a grueling photoshoot.
We started at about 10 am and finished around 4pm and I was completely spent, but the more we shot the sharper I looked, so we kept on going.
It's nice to look back from time to time and as tired as I was, we all had a blast!
My thanks to @stephanie_corne_artwork, @https://pulse.ly/itgnag2dec and @ftaz1 for taking the shots!!!
Thanks for watching and as always, Excelsior!!! #naturallyintense
#naturalbodybuilder #naturalbodybuilding #throwback #fifthavenuegym #5thavenuegym #drugfreebodybuilding #naturalbodybuildinglifestyle #gymlife #gymmotivation #naturalbodybuildingmotivation #bodybuilding #blackandwhite #instablackandwhite #bnw
{kind=link}
Can You Build An Impressive Physique Training Only At Home?
Absolutely!
I stopped training in commercial gyms as of March 2020 and have been training at home ever since.
Initially I was admittedly worried that I might lose some of my gains or not make as much progress, but that certainly wasn't the case.
I've consistently continued to improve with my high intensity workouts and muscles have no idea where they are training.
As long as the criteria of adequate intensity and overload are met, there will be an adaptive response and your muscles will get bigger and stronger.
So don't worry at all about where you train, focus instead of what will be the best way for you to always be training!
Thanks for watching and as always, Excelsior!!! #naturallyintense
{kind=link}
Kevin's Three Day Training Spilt!
For the past 33 years I have trained three times a week with Naturally Intense High Intensity Training workouts lasting 10, 15 to 20 minutes max.
It's a training split tried and testes not only in it's helping me realize my goal of becoming a successful natural bodybuilder, but it's also helped hundreds of men and women over the past three decades.
I have tested just about every possible training split imaginable and for this particular style of high intensity training, this particular grouping consistently yields fantastic results.
I hope it helps you as much as it's helped me over the years and thanks so much for taking the time to look at my work.
Keep training hard and Excelsior!!! #naturallyintense
Excelsior!!! #naturallyintense
#trainingsplit #3daytrainingsplit #threedaytrainingsplit #naturalbodybuilding #naturalbodybuilder #naturalbodybuildingvideo #naturalbodybuildingmotivation #naturalbodybuildingtips #drugfreebodybuilding #bodybuilding #highintensitytraining #highintensitytrainingtips
{kind=link}
405 Stiff Leg Deadlift for 7 Reps! High Intensity Training.
First leg workout of the year and already pushing it!
I haven't done a stiff leg deadlift over 315lbs for about 3 years at this point, and I did my last set with 315lbs and comfortably got to 10 reps and decided I had far too much gas left in the tank and that I should go up in weight.
So I did.
I figured I might get a solid 6 reps in, but I made it to 7 and I think I could have gone on to get a full 10 reps BUT that's when good judgement prevailed.
As a bodybuilder having not trained this heavy for so many years, the shock of this much weight would be more than enough to stimulate muscle growth, and doing more reps wouldn't yield any greater returns, only increase the likelihood of injury.
It's not about the numbers, it's about training to a point where you achieve your goal, and it's important to have a goal in mind as a bodybuilder based on increasing muscle mass rather than hitting a particular number.
Besides, if in my 20's I never did more than 405lbs on a stiff leg deadlift, it doesn't make any sense going heavier than when I am almost 50!
Could I deadlift more at this point?
Absolutely but just because you can doesn't mean you should!
So keep those weights in a good working range, keep it safe and as always Excelsior!!! #naturallyintense
#hometraining #homeworkout #homeworkout #roguerack #highintensitytraining #naturalbodybuilder #naturalbodybuilding #fitover40 #naturalbodybuildingvideos #backworkout #naturalbodybuildingtips #backtraining #highintensitytrainingtips #drugfreebodybuilding #fitoverforty #deadlift
{kind=link}
Turning 50 in a few months...
Not much of a big deal for me as I still feel pretty much the same but I hope that my example helps show what can be done with a lifetime commitment to eating well and training consistently!
Thanks for coming along on the journey and as always, Excelsior!!! #naturallyintense
#naturalbodybuilder #naturalbodybuilding #healthylifestyle #fitover40 #drugfreebodybuilding #naturalbodybuildingmotivation #natty #fitness
Please note that all material is copyrighted and DMCA Protected and can be reprinted only with the expressed authorization of the author.
Related Articles:
Exercise As A Tool For Relieving Depression
The Spiritual Side of Bodybuilding
Please note that all material is copyrighted and DMCA Protected and can be reprinted only with the expressed authorization of the author.
Featured everywhere from the Wall Street Journal to CBS News, Kevin Richardson’s Naturally Intense High Intensity Training have helped hundreds lose weight and transform their bodies with his 10 Minute Workouts. One of the top natural bodybuilders of his time, Kevin is also the international fitness consultant for UNICEF and one of the top personal trainers in New York City.
References Exercise Addiction: Understanding How & Why It Happens:
- De Coverley Veale, D.M. Exercise addiction. Br. J. Addict. 1987,
- Cook, B.; Hausenblas, H.; Tuccitto, D.; Giacobbi, P.R., Jr. Eating disorders and exercise: A structural equation modeling: Analysis of a conceptual model. Eur. Eat. Disord. Rev. 2011
- Freimuth, M. Addicted? Recognizing Destructive Behavior before It’s too Late; Rowman & Littlefield Publishers, Inc: Lanham, MD, USA, 2008.
- Thornton, E.W.; Scott, S.E. Motivation in the committed runner: Correlation between self-report scales and behavior. Health Promot. Int. 1995
- Scully, D.; Kremer, J.; Meade, M.M.; Graham, R.; Dudgeon, K. Physical exercise and well-being: A critical review. Br. J. Sports Med. 1998
- McNeil K, LeBlanc E, Joyce M. The effect of exercise on depressive symptoms in the moderately depressed elderly. Psychology of Aging 1991
- Blumenthal JA, Babyak MA, Moore KA, et al. Effects of exercise training on older patients with major depression. Archives of Internal Medicine 1999
- Singh NA, Clements KM, Fiatarone MA. A randomized controlled trial of progressive resistance training in depressed elders. Journal of Gerontology Medical Sciences
- Doyne EJ, Ossip-Klein DJ, Bowman ED, Osborn KM, McDougall-Wilson IB, Neimeyer IB. Running Versus Weight Lifting in the Treatment of Depression. Journal of Consulting and Clinical Psychology. 1987
- Martinsen EW, Hoffart A, Solberg O. Comparing aerobic and non aerobic forms of exercise in the treatment of clinical depression: a randomized trial. Comprehensive Psychiatry 1989
- Craft, L.L.; Perna, F.M. The benefits of exercise for the clinically depressed. Prim. Care Companion J. Clin. Psychiatry 2004
- Stahl, S.M. Stahl’s Essential Psychopharmacology: Neuroscientific Basis and Practical Applications, 3rd ed.; Cambridge University Press: New York, NY, USA, 2008
- Rosa, D.A.; De Mello, M.T.; Negrao, A.B.; De Souza-Formigoni, M.L.O. Mood changes after maximal exercise testing in subjects with symptoms of exercise dependence. Percept. Mot. Skills 2004
- Zmijewski, C.F.; Howard, M.O. Exercise Addiction and attitudes toward eating among young adults. Eat. Behav. 2003
- Johnston, O.; Reilly, J.; Kremer, J. Excessive exercise: From quantitative categorisation to a qualitative continuum approach. Eur. Eat. Disord. Rev. 2011
- Sussman, S.; Lisha, N.; Griffiths, M. Prevalence of the addictions: A problem of the majority or the minority? Eval. Health Prof. 2011
- Allegre, B.; Therme, P.; Griffiths, M. Individual factors and the context of physical activity in exercise dependence: A prospective study of “ultra-marathoners”. Int. J. Ment. Health Addict 2007.
- Terry, A.; Szabo, A.; Griffiths, M. The exercise addiction inventory: A new brief screening tool. Addict. Res. Theory 2004
- Lejoyeux, M.; Avril, M.; Richoux, C.; Embouazza, H.; Nivoli, F. Prevalence of exercise addiction and other behavioral addictions among clients of a Parisian fitness room. Comprehensive Psychiatry 2008
- Carnes, P.J.; Murray, R.E.; Charpentier, L. Bargains with chaos: Sex addicts and addiction interaction disorder. Sexual Addiction and Compulsivity 2005
- Haylett, S.A.; Stephenson, G.M.; LeFever, R.M.H. Covariation of addictive behaviors: A study of addictive orientation using the Shorter Promis Questionnaire. Addict. Behav. 2004
- MacLaren, V.V.; Best, L.A. Multiple addictive behaviors in young adults: Student norms for the Shorter PROMIS questionnaire. Addict. Behav. 2010
- Aidman, E.V.; Woollard, S. The influence of self-reported exercise addiction on acute emotional and physiological responses to brief exercise deprivation. Psychol. Sport Exerc. 2003
- George, A.J. Central nervous system stimulants. Best Practice & Research Clinical Endocrinology & Metabolism 2000
- National Institute on Drug Abuse. InfoFacts: Steroids (Anabolic-Androgenic); National Institutes of Health: Washington, DC, USA, 2009
- Hakansson A, Mickelsson K, Wallin C, Berglund M. Anabolic androgenic steroids in the general population: user characteristics and associations with substance use. Eur Addict Res. 2012
- EJ, Barnett MJ, Tenerowicz MJ, Perry PJ. The Anabolic 500 survey: characteristics of male users versus nonusers of anabolic-androgenic steroids for strength training. Pharmacotherapy. 2011
- Hausenblas, H.A.; Downs, D.S. How much is too much? The development and validation of the Exercise Addiction scale. Psychology and Health 2002
- Bamber, D.J.; Cockerill, I.M.; Rodgers, S.; Carroll, D. Diagnostic criteria for exercise addiction in women. Br. J. Sports Med. 2000
- Friemuth M, Moniz S., Kim S.R. Clarifying Exercise Addiction: differential diagnosis, co-occurring disorders, and phases of addiction. Int. J. Environ. Res. Public Health 2011
- An Overview of Activity Anorexia. In Activity Anorexia: Theory, Research, and Treatment; Epling, W.F., Pierce, W.D., Eds.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1996
- O’Dea, J.A.; Abraham, S. Eating and exercise disorders in young college men. J. Am. Coll. Health 2002
- Griffiths, M.D. A “components” model of addiction within a biopsychosocial framework. J. Subst. Use 2005
- Johnston, O.; Reilly, J.; Kremer, J. Excessive exercise: From quantitative categorization to a qualitative continuum approach. Eur. Eat. Disord. Rev. 2011
- Freimuth, M. Addicted? Recognizing Destructive Behavior before It’s too Late; Rowman & Littlefield Publishers, Inc: Lanham, MD, USA, 2008
- Griffiths, M. Exercise addiction: a case study. Addict. Res. 1997
- Klein, D.A.; Bennett, A.S.; Schebendach, J.; Foltin, R.W.; Devlin, M.J.; Walsh, B.T. Exercise “addiction” in anorexia nervosa: Model development and pilot data. CNS Spectrums 2004